Casos de Éxito
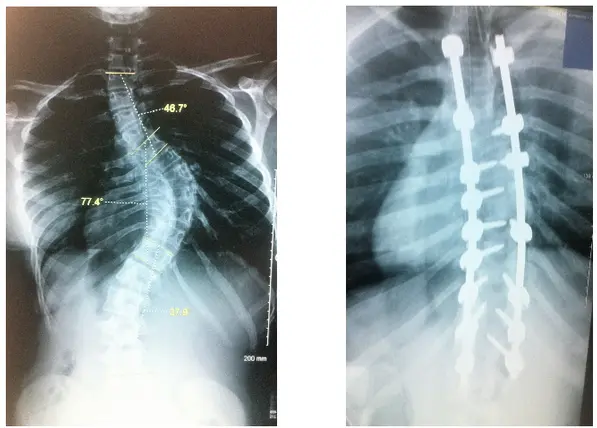
13-year-old female patient.
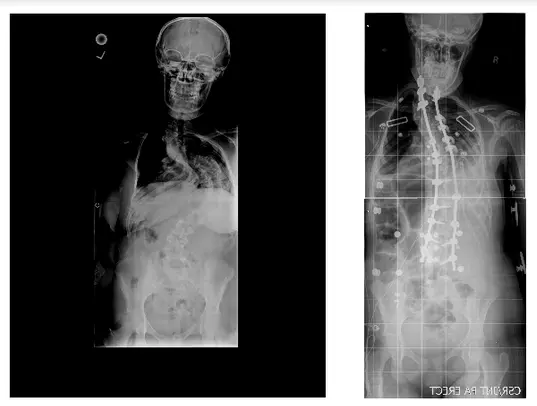
Diagnosed with adolescent idiopathic scoliosis, her deformity was gradually progressive until requiring a surgical solution. Her curves were 46 degrees, 77 degrees, and 36 degrees.
Surgical correction was performed with screws and bars in the spine. The result was very satisfactory and the aesthetic appearance improved significantly..
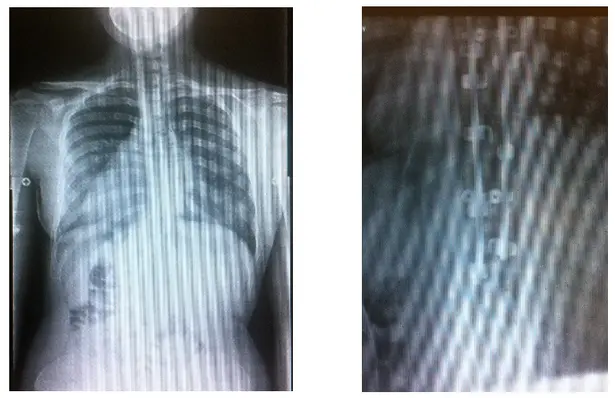
15-year-old female patient.
Diagnosed with adolescent idiopathic scoliosis, her deformity was gradually progressive until requiring a surgical solution. Her curve was 50 degrees, very flexible.
The surgical correction was performed with hooks and bars in the spine. The patient had a very satisfactory result, with a very adequate improvement in the physical aspect according to the family and with herself.
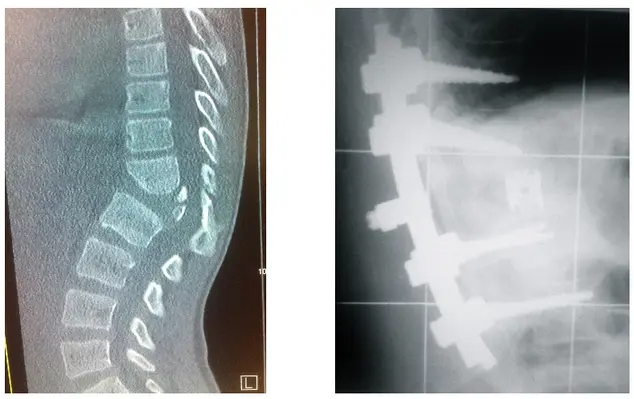
Male patient, 9 years old.
Diagnosed with a T12 vertebral body hemivertebra. His congenital malformation triggered a kyphotic deformity of the spine. He required surgical treatment due to curve progression.
Surgical correction was performed posteriorly only, with pediatric size screws and bars in the spine, also requiring a spacer between the vertebral bodies. The result was very satisfactory and the spinal deformity was corrected.
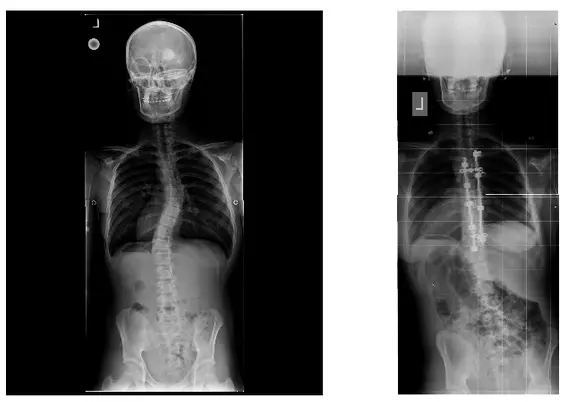
Female patient, 11 years old.
Diagnosticada con escoliosis idiopática del adoslecente, su deformidad fue gradualmente progresiva hasta requerir una solución quirúrgica; esta paciente rehusó el uso del corset en todo momento. Su curva era de 44 grados.
Female patient, 14 years old.
Surgical correction consisted of multiple procedures, both anteriorly through the thorax and posteriorly. The final correction was 70% of the size of the original curves, with a significant improvement in pulmonary function.

61-year-old female patient.
Diagnosed with flat spine syndrome, adult degenerative scoliosis and multilevel spinal stenosis, manifested by severe low back pain, gait claudication and sciatica.
The surgical correction consisted of 2 procedures, both anteriorly, through the abdomen, and posteriorly. Note the improvement of the lumbar spine curvature, recovery of the height of the collapsed intervertebral discs, correction of the scoliosis, correction of the sagittal balance, in addition to an adequate decompression of the pinched nerves.
56-year-old female patient.
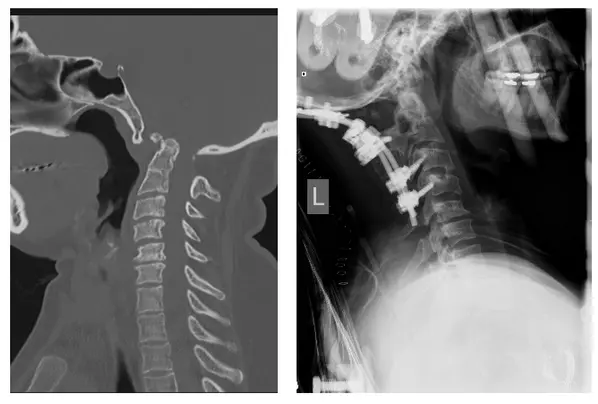
Diagnosed with a basilar invagination (note how the cervical spine inserts into the foramen where the cerebrum and cerebellum are located). The patient developed paralysis of her extremities within 2 months, with great difficulty walking.
Surgical stabilization consisted of a correction of the invagination with the use of cervical traction and then proceeding with fusion surgery and subsequent cervical instrumentation..

37-year-old female patient.
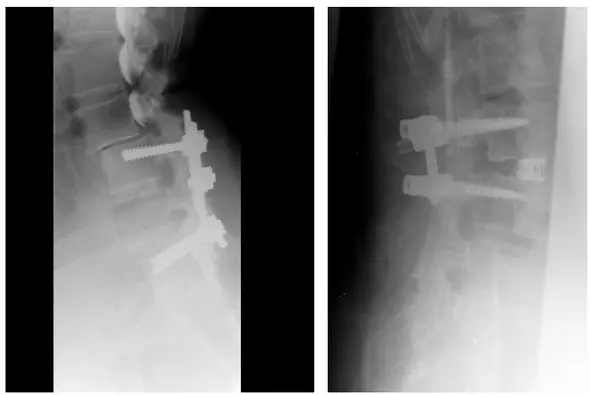
Diagnosed with L5-S1 GIII spondylolisthesis, manifested by severe low back pain, gait claudication and sciatica.
Surgical correction consisted of a posterior approach. He underwent fusion and instrumentation from L4 to S1 and iliac crests, in addition to the placement of a spacer between the vertebral bodies. All for the purpose of stabilization, fusion, recovery of the normal lumbar curve, elevation of the collapsed intervertebral space, and decompression of the pinched nerves.

Female patient, 73 years old.
Diagnosed with flat spine syndrome, adult degenerative scoliosis and multilevel spinal stenosis, manifested by severe low back pain, gait claudication and sciatica.
Surgical correction consisted of 2 procedures, both anteriorly, through the abdomen, and posteriorly. Note the partial improvement of the lumbar spine curvature, recovery of the height of the collapsed intervertebral discs, partial correction of the scoliosis, correction of the sagittal balance (note the head better positioned over the pelvis), in addition to an adequate decompression of the pinched nerves.
Male patient, 54 years old.
With a history of spinal fusion surgery and spinal instrumentation about 9 years ago. She consulted the doctor due to progressive low back pain until it became incapacitating.
He was diagnosed with degeneration of the segment adjacent to the previous fusion with a spondylolisthesis (note how the lumbar spine appears displaced forward).
Surgical correction consisted of a posterior approach procedure. The patient underwent removal of the previous metallic material, exploration of the previous fusion surgery, and fusion and instrumentation of the adjacent segment with placement of a spacer between the vertebral bodies. All for the purpose of stabilization, fusion, recovery of normal curvature, and elevation of the collapsed intervertebral space.